


Frequently Answered Questions
2. Injected versus ingested aluminium

There is no discussion. Aluminium administered in a vaccine or in immunotherapy is an acute exposure to aluminium. By comparison, exposure to aluminium through the gut might be considered as chronic. The terms acute and chronic are defined in this instance in that an acute response elicits an immediate response to the presence of aluminium while this would not necessarily be the case for chronic exposure. The movement of aluminium across the gut epithelium is fraught with difficulty as identified in the figure below.
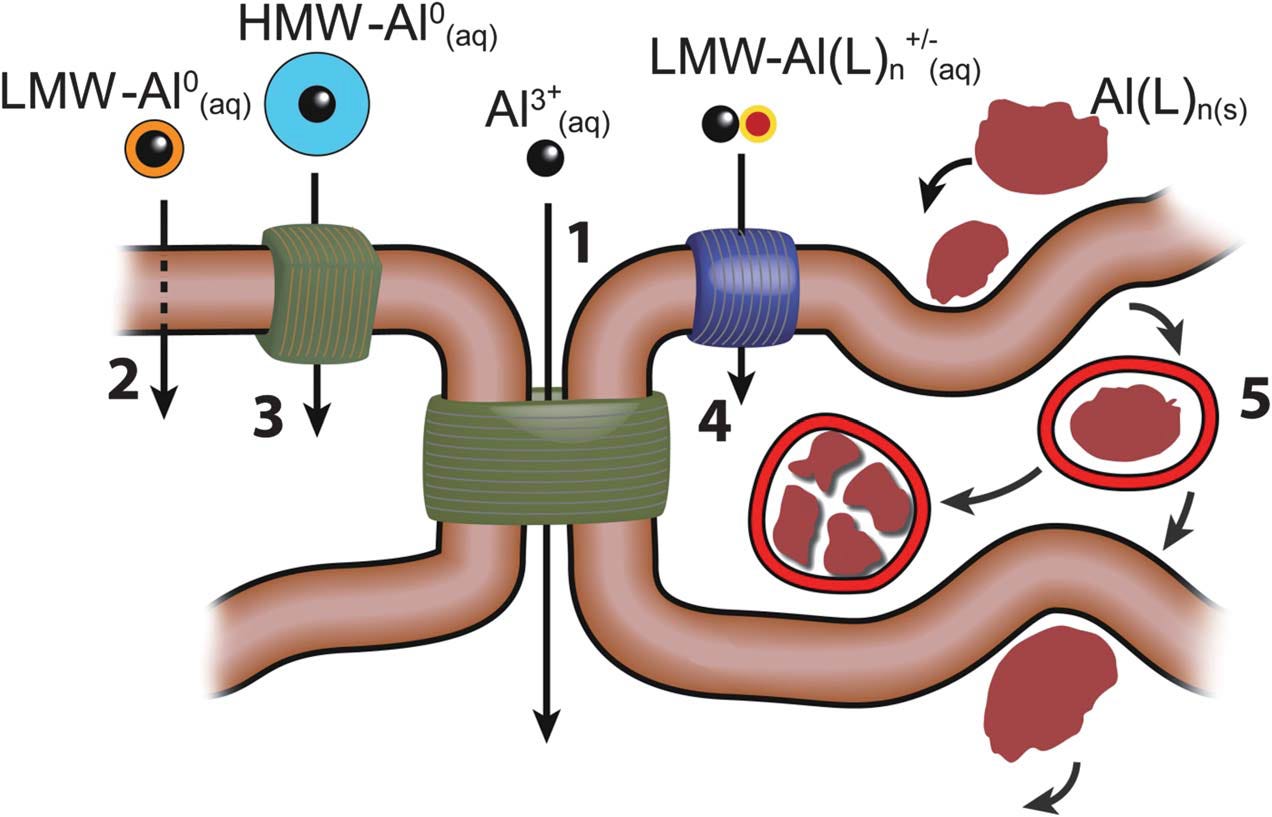
The diagram shows that there are 5 major routes by which aluminium could be transported across cell membranes or cell epi-/endothelia; (1) paracellular; (2) transcellular; (3) active transport; (4) channels; (5) adsorptive or receptor-mediated endocytosis. There are 5 major classes of forms of aluminium which could participate in these transport routes. These are shown in the figure as; the free solvated trivalent cation (Al3+(aq)); low molecular weight, neutral, soluble complexes (LMW-Al0(aq)); high molecular weight, neutral, soluble complexes (HMW-Al0(aq)); low molecular weight, charged, soluble complexes (LMW-Al(L)n+/-(aq)); nano and micro-particulates (Al(L)n(s)).
The published data relating to the proportion of ingested aluminium that will eventually pass through the gut epithelium and into the blood is unreliable at best but can be estimated as between 0.1 and 10%. Aluminium entering the blood must then pass through the liver where a significant, but again data are unreliable, proportion will be removed and excreted back into the gut via bile. Human exposure to aluminium through ingestion should be considered as a type of slow release system involving only an insignificant proportion of aluminium entering the gut.
Now compare this to exposure to aluminium as an aluminium adjuvant in a vaccine or immunotherapy. Take a close look at what is happening at the injection site.
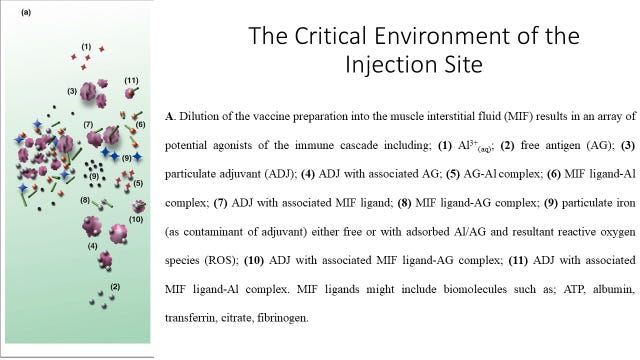
The body is immediately challenged by an acute exposure to aluminium. You know that it is acute because there is an almost immediate inflammatory response, the red mark at the injection site. Of the myriad ways that aluminium can react at the injection site it is the action of the free metal cation (Al3+(aq)) in bringing about cell death through necrosis that is responsible for the inflammation. I have also argued that this toxicity at the injection site is the main mechanism of action of aluminium adjuvants in boosting the immune response.
Note that unlike exposure to aluminium through ingestion all of the injected aluminium has access to the blood and this aluminium may also impact upon major organs such as the brain without first encountering the detoxification brought about by the liver.
Critically, both to the success of aluminium salts as adjuvants but similarly to the toxicity of aluminium beyond the injection site, the toxicity of aluminium instigates the infiltration of the injection site by many different immunocompetent cells. Huge numbers of hungry phagocytic cells invade the injection site and begin to clear away aluminium adjuvant by engulfing it and storing it in vesicles in their cytoplasm. Macrophages are one such cell type and the image below shows how they accumulate aluminium (showing as a fluorescent red colour) in their cell bodies.

This remarkable image shows how macrophages gorge upon aluminium adjuvants. However, what it doesn’t tell us is what happens next. The macrophages retain their viability for days, weeks and possibly months. This enables them as vehicles for the transport of significant amounts of aluminium throughout the body. At some point their toxic cargo of aluminium will kill them and they will deposit their aluminium in the tissue or compartment in which they met their demise. The cycle of toxicity may then continue with the deposited aluminium bringing about further cell death and inflammation. If this happened to be in the brain tissue of an infant then it might even be likened to an injection of aluminium adjuvant directly into brain tissue. Therein lies a major concern about aluminium adjuvants in vaccines and immunotherapy and distinguishes their potential toxicity from ingested aluminium.
Next time you are confronted with this question have no doubt in your mind that injected aluminium is an acute exposure in comparison to aluminium in the diet. The acuity of such an exposure is, of course, significantly greater for an infant as compared to an adult. It is time that we stopped using aluminium adjuvants full stop.
It is time that ALL vaccines were stopped. Then never be permitted into use until there was pure scientific evidence that they are better than never having them. In the US, rescinding the 1986 vaccines laws would be a great start.
As always, EXCELLENT information! THANK YOU! I will be forwarding this post to two of my doctors.